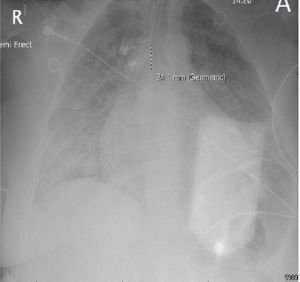
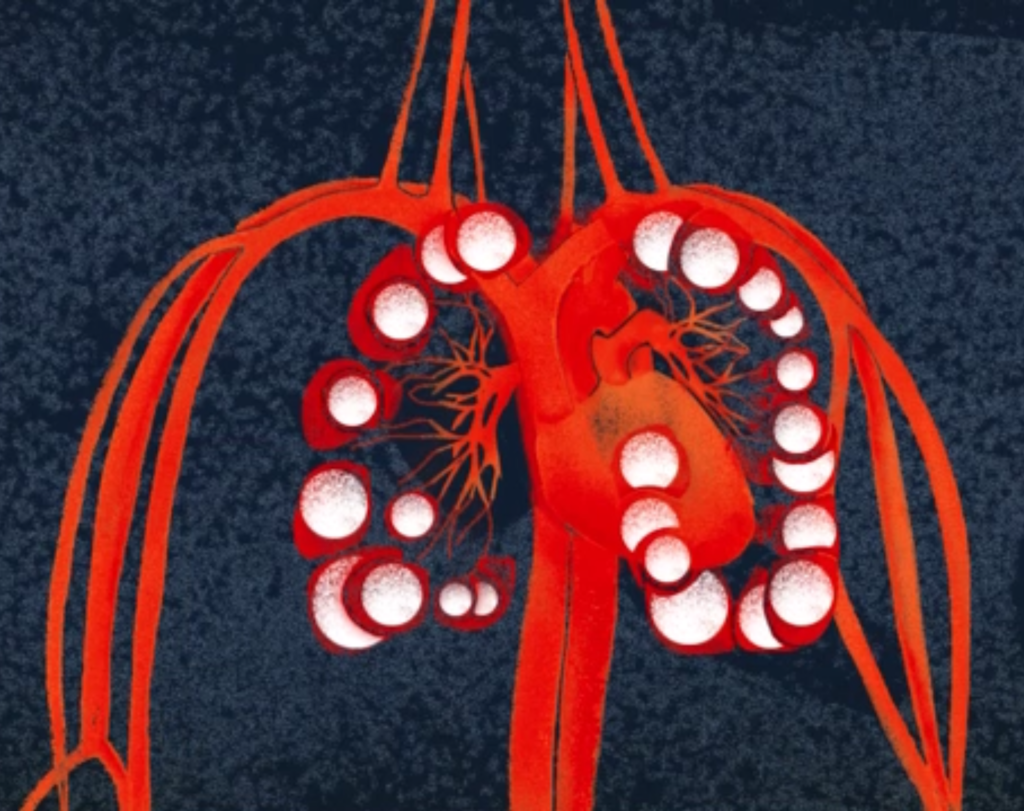
Patients that go into cardiac arrest after a seizure and are successfully resuscitated for at least one hour are said to have experienced a “near SUDEP” event. I had such a patient in 2023. She had suffered intermittent epileptic seizures most of her life but never pursued medical care. Thus, she would have met “probable” SUDEP criteria had she not been resuscitated. The severity of her pulmonary edema and its correlation with transiently increased white blood cell counts suggest that her seizures triggered a surge of systemic catecholamines that likely precipitated her sudden and unexpected demise